J Transcat Intervent.2023;31:eA20220015.
Intravascular ultrasound in percutaneous coronary intervention guidance: results from Portuguese registry
Carla Maria Marques Pires Rodrigues
![]() , Carlos Galvão Braga
, Carlos Galvão Braga
![]() , Marco Costa, Pedro Canas da Silva, Rui Cruz Ferreira, Rui Campanhe Teles, João Carlos Silva, Filipe Seixo, João Costa
, Marco Costa, Pedro Canas da Silva, Rui Cruz Ferreira, Rui Campanhe Teles, João Carlos Silva, Filipe Seixo, João Costa
![]() , Hélder Pereira, Pedro Pinto Cardoso, Eduardo Infante de Oliveira
, Hélder Pereira, Pedro Pinto Cardoso, Eduardo Infante de Oliveira
DOI: 10.31160/JOTCI202331A20220015
ABSTRACT
Background
Current guidelines recommend the use of coronary intravascular ultrasound as an adjunctive tool in challenging situations.
Objective
To characterize the use of intravascular ultrasound in Portugal and compare outcomes after left main percutaneous coronary intervention, with or without intravascular ultrasound.
Methods
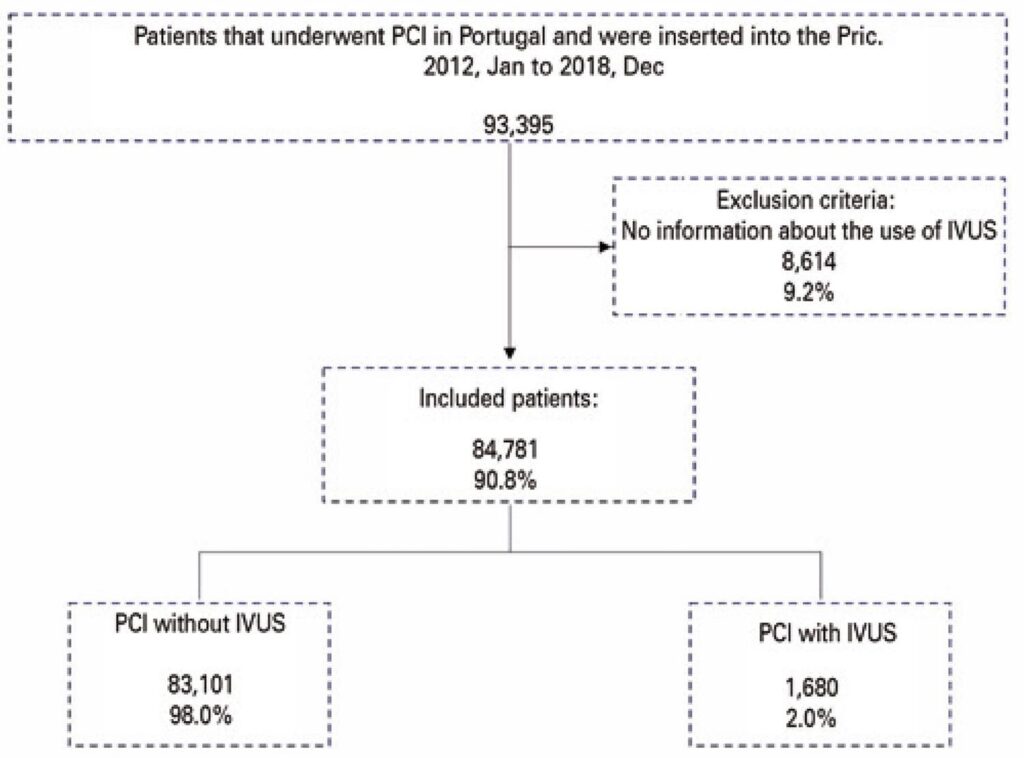
A retrospective multicentric observational study analyzed patients who underwent percutaneous coronary intervention between January 2012 and December 2018 and were included in the Portuguese Registry on Interventional Cardiology of the Sociedade Portuguesa de Cardiologia . A two-sided p-value<0.05 was considered statistically significant.
Results
This study revealed significant variation of intravascular ultrasound usage in Portugal over time (p-value Chi-squared for trend <0.001). The year with maximum use was 2016 (2.4%). Regarding left main percutaneous coronary intervention, there was a progressive increase in use of intravascular ultrasound (p-value Chi-squared for trend<0.001) in the last 7 years, with important regional differences. The population submitted to left main percutaneous coronary intervention with intravascular ultrasound was younger, but had a higher prevalence of some cardiovascular risk factors, ventricular systolic dysfunction, and complex coronary lesions. Moreover, this group of patients had lower prevalence of intrahospital primary endpoint (1.4% versus 3.9%; p=0.024). However, after multivariate analysis adjusted to confounding factors, this study did not demonstrate a significant impact of intravascular ultrasound on intrahospital endpoint.
Conclusion
The overall use of intravascular ultrasound in left main percutaneous coronary intervention has been slowly increasing in the last seven years, in Portugal. In this study, the use of this method had no statistical impact in intrahospital endpoints.
240