Risk awareness of no-reflow is mandatory, especially in patients with cardiovascular risk factors, long door-to-balloon time, and in the presence of angiographic evidence of a large thrombus burden. Some preventive strategies have been described. Nevertheless, in clinical practice, is difficult to avoid no-reflow. Interventional cardiologists have no guidelines or recommendations for this situation. We suggest that a conservative management with dual antiplatelet therapy and slow intravenous infusion of nitroglycerine over 12 to 24 hours and abciximab, followed by deferred re-evaluation days later could be a good strategy for refractory no-reflow.
Refractory no-reflow phenomenon. Keep calm and watchful waiting!
López-Lluva,María Thiscal and Jurado-Román,Alfonso and Sánchez-Pérez,Ignacio and Abellán-Huerta,José and Piqueras-Flores,Jesús and Maseda-Uriza,Ramón and Ruíz-Poveda,Fernando Lozano. Refractory no-reflow phenomenon. Keep calm and watchful waiting!. J Transcat Intervent. [online]. 2019, vol.27, [cited 2026-06-23], Available from: <https://jotci.org/article/refractory-no-reflow-phenomenon-keep-calm-and-watchful-waiting/>. ISSN . https://doi.org/10.31160/JOTCI201927A20180005.
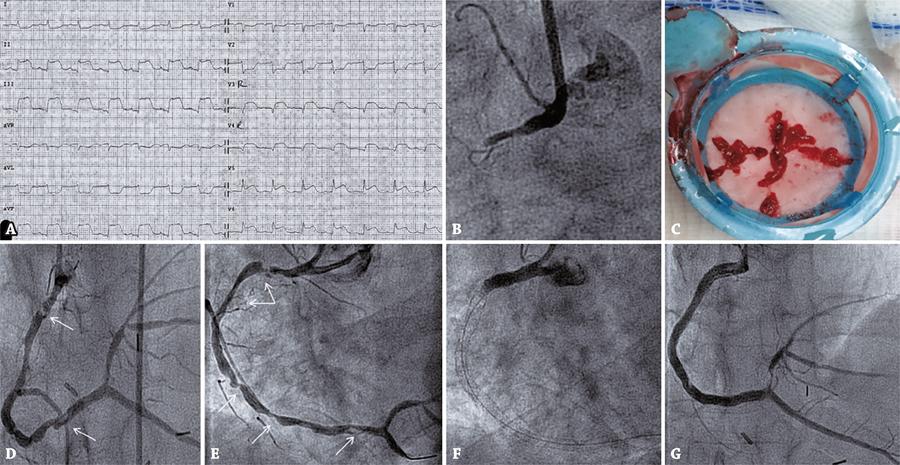
No-reflow after primary percutaneous coronary intervention in a patient presenting with acute inferior myocardial infarction. (A) Electrocardiogram performed at first medical contact demonstrating inferolateral ST-segment elevation acute myocardial infarction with reciprocal images. (B) Coronary angiography showing an acute total occlusion of the proximal right coronary artery. (C) Red thrombi obtained by thrombus aspiration. (D) Angiography revealing thrombus-like filling defect in the proximal and distal portion of right coronary artery (white arrows). (E) Diffusely diseased right coronary artery, with multiple severe calcified lesions (white arrows). (F) Left anterior oblique view presenting no-reflow phenomenon of right coronary artery. (G) Angiography done 1 week later exhibiting TIMI-3 flow at right coronary artery and stents patency, with residual thrombus in mid right coronary artery and proximal posterolateral branch.