J Transcat Intervent.2022;30:eA20210040.
The impact of percutaneous coronary intervention versus coronary artery bypass grafting surgery in left main coronary artery disease – a single center experience
Cátia Costa Oliveira
![]() , Ana João Guerra
, Ana João Guerra
![]() , João Costa
, João Costa
![]() , Carlos Galvão Braga
, Carlos Galvão Braga
![]() , Jorge Marques
, Jorge Marques
![]()
DOI: 10.31160/JOTCI202230A20210040
ABSTRACT
Background:
Although coronary artery bypass grafting has been considered the gold-standard treatment for stable ischemic left main coronary artery disease, percutaneous coronary intervention has shown good results, and is an alternative to surgery. This study aimed to evaluate and compare a real-world population with stable left main coronary artery disease submitted to coronary artery bypass grafting or percutaneous coronary intervention, regarding their characteristics and outcomes.
Methods:
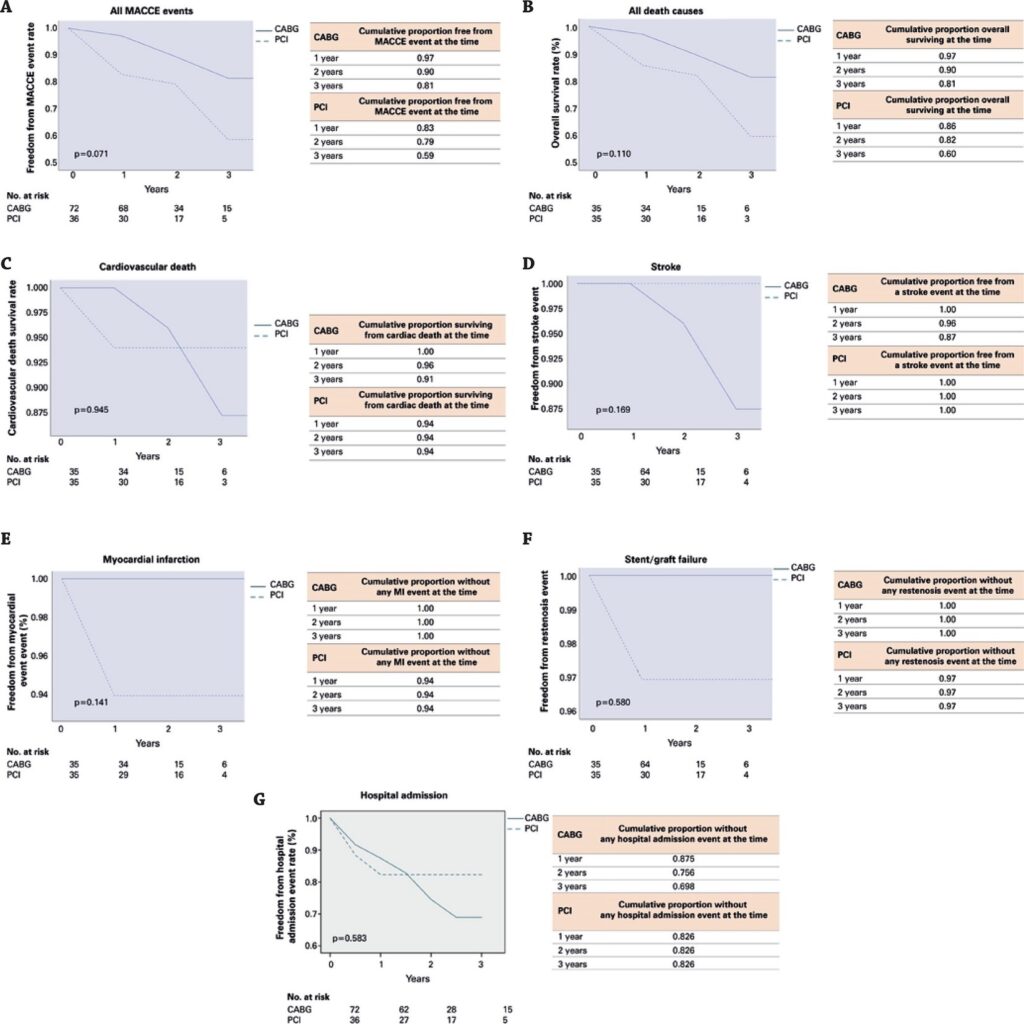
Two samples of patients with stable ischemic left main coronary artery disease, who underwent coronary artery bypass grafting or percutaneous coronary intervention between January 2015 and November 2018, were evaluated and their clinical outcomes compared. The cumulative event rates were based on the Kaplan-Meier curve and compared with log-rank statistics. Hazard ratio and 95%CI and p-values, were obtained through univariate Cox regressions.
Results:
No significant differences were found between the percutaneous coronary intervention and coronary artery bypass grafting groups in the total composition of risks for major cardiac and cerebrovascular events (hazard ratio of the percutaneous coronary intervention group of 2.066; 95%CI 0.876-4.869; p=0.097) or in the risk of death from cardiovascular cause (hazard ratio for the percutaneous coronary intervention group of 1,117; 95%CI 0.204-6,109; p=0.898). However, the group classified as high coronary artery disease anatomical complexity had worse results regarding major cardiac and cerebrovascular events rates when submitted to percutaneous coronary intervention (hazard ratio of 2.699; 95%CI 1.002-7.266; p=0.049).
Conclusion:
The results obtained suggest that both treatments are valid options for the treatment of stable ischemic left main coronary artery disease, except in patients with high coronary anatomic complexity, in whom coronary artery bypass grafting should remain the treatment of choice.
270