J Transcat Intervent.2022;30:eA2021000039.
When the answer was already there
Carla Maria Marques Pires Rodrigues
![]() , Jorge Marques
, Jorge Marques
![]() , Carlos Galvão Braga
, Carlos Galvão Braga
![]()
DOI: 10.31160/JOTCI202230A20210039
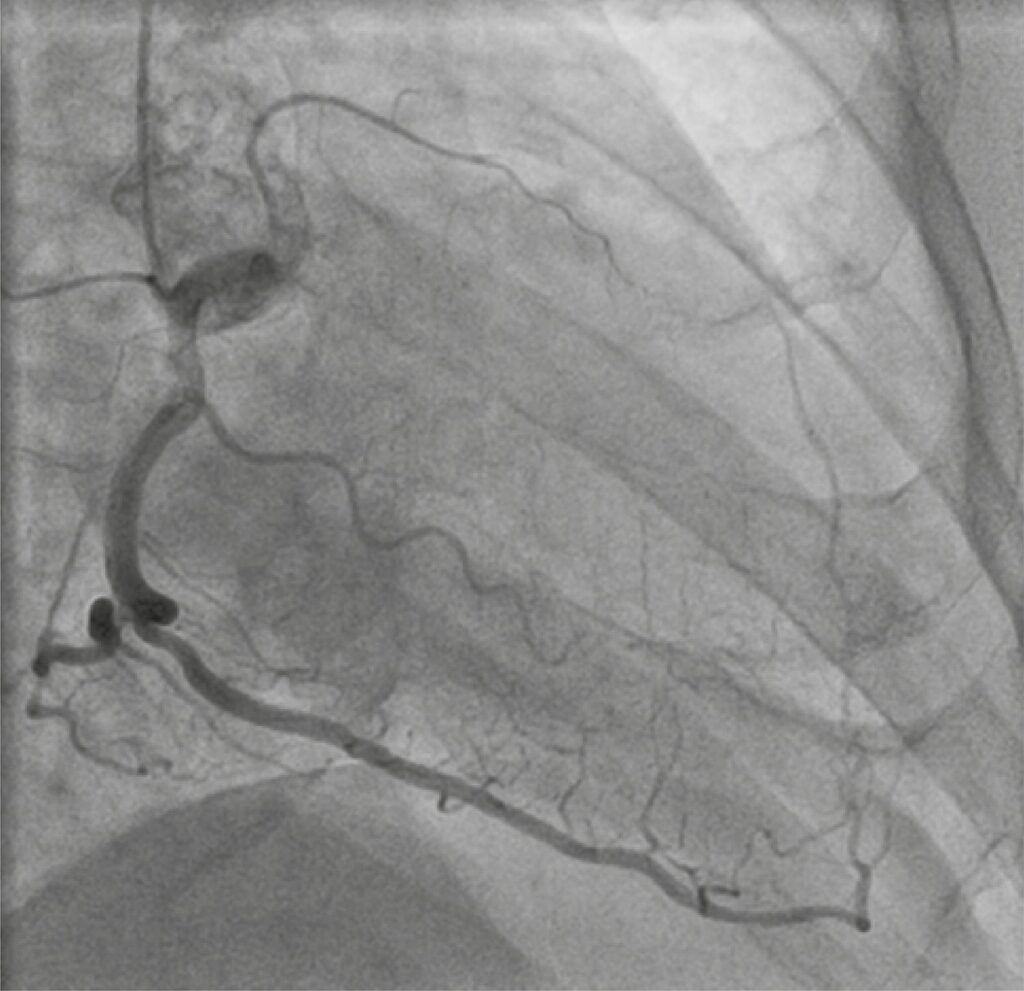
A 67-year-old man with several cardiovascular risk factors was referred to cardiology consultation, due to effort angina – Canadian Cardiology Society (CCS) class II/IV, for the last 6 months, under optimal medical treatment. Resting electrocardiogram and transthoracic echocardiogram (TTE) were normal. Stress treadmill test was positive. The coronary angiogram revealed a long proximal chronic total occlusion (CTO) of the left anterior descending artery (LAD; J-CTO=1, Rentrop3), a distal CTO of the left circumflex artery (J-CTO=0, Rentrop3) and a 50% stenosis in the posterolateral branch (SYNTAX score 21).
Considering symptoms, angiographic findings, and patient preference, a percutaneous coronary intervention (PCI) of LAD was planned, as priority, and performed using bi-radial access, contralateral injection, and anterograde wire escalation approach ( ). Sion guidewire was advanced to distal LAD with the aid of FineCross microcatheter . Two overlapping everolimus-eluting stents (2.5x48mm and 3x23mm) were deployed in proximal LAD, after adequately pre-dilatation. Immediately after post-dilatation with non-compliant balloon (3x23mm) at 22atm, the patient developed a severe Ellis type III perforation in the mid LAD (). The post-dilatation balloon was re-inflated at 8atm, at the site of perforation to stop bleeding. A bedside TTE was performed and revealed small circumferential pericardial effusion without hemodynamic impact.
[…]
181